


Dementia is a clinical syndrome caused by neurodegeneration and characterized by progressive deterioration in cognition and capacity for independent living.1 It has been described as a global epidemic.2 The occurrence of dementia in low- and middle-income countries (LMICs) is closely linked to population ageing and thus may continue to rise for decades.2,3 Globally, about 47.5 million people are living with dementia, with over two-thirds residing in LMICs, including Africa, where there is very limited access to social protection, and relevant care, services and support.1
Documented country-specific dementia prevalence in sub-Saharan Africa (sSA) ranges between 2% and 5%. 4,5 Although in most of these settings, dementia research is relatively poor; consequently, the awareness and response to dementia have been limited.6 In Nigeria, several communities still link dementia to a normal process of ageing, with many patients stigmatised and abandoned in the belief that their condition is beyond any medical intervention.7 Thus, many of those affected delay seeking medical care and endure poor outcomes.8 This is exacerbated by poor mental health service access which partly results in high out-of-pocket expenses that few can afford.9,10
The Ibadan study of ageing group,10–12 covering several parts of the south-west Nigeria, is widely recognized as a leading research group on dementia in Nigeria. The group over the last two decades, has contributed to the understanding of the burden of dementia in the south-west region. However, the remaining five of the six geopolitical zones in the country lack recent epidemiologic data. Population-based research studies on dementia have been sparsely conducted in Nigeria,6 a view already reported by the 10/66 dementia research group for several LMICs.13 Prince and colleagues,6 however, called for increased efforts towards gathering available research evidence on the burden of dementia to further raise awareness on the numbers of people affected and inform relevant policy interventions. We therefore systematically reviewed available evidence on dementia in Nigeria to provide estimates of the prevalence and risks of dementia that can subsequently prompt a much-needed policy response and country-wide public health interventions.
METHODS
Search strategy
We searched relevant databases, including MEDLINE, EMBASE, Global Health (CABI), and Africa Journals Online (AJOL), for epidemiologic studies on dementia in Nigeria. Search terms are shown in Table 1. Searches were conducted on 31 July 2018 and limited to studies published after 1 January 1990. Unpublished documents were sourced from Google Scholar and Google searches. Titles and abstracts of studies were reviewed, and full-texts of relevant studies accessed. The reference lists of accessed full-texts were further hand-searched for additional studies. The authors of selected papers were contacted for missing information.
Selection criteria
We primarily selected population-based studies reporting on the prevalence or risks of dementia in a Nigerian setting. However, due to high number of hospital-based studies we identified from an initial scoping exercise reporting risks of dementia, we also carefully reviewed and selected hospital-based studies if they clearly defined the reference population of the hospital (which we ascertained by checking with the authors or relevant authorities of the hospital). We excluded any other hospital-based studies with poor or no description of reference population. Other studies excluded include studies on Nigerians in diaspora, reviews, case-reports, view-points and commentaries.
Data extraction
Assessment of eligible studies was conducted independently by two reviewers (DA and AA), with an eligibility guideline to ensure that selection consistent criteria were applied. Any disagreement in study selection was resolved by consensus. Data on the location, study period, study design, study setting (urban or rural), sample size, diagnostic criteria and mean age of the population were extracted. These were matched with corresponding data on dementia cases, sample population, prevalence, and estimated risks of dementia in each study. For studies conducted on the same study site, population or cohort, the first published study was selected, and all additional data from the other studies were extracted and merged with data from the selected paper.
Quality assessment
For the quality assessment, we adapted the Alzheimer’s Disease International study selection and quality criteria.1 For each full text selected, we screened for adherence to protocol in the study design (was there a protocol?), sampling method (was it representative of a target subnational population?), and case ascertainment (was it based on standard diagnostic criteria, measurement of cognitive impairment or unspecified clinical criteria, informant interviews, or not reported?). Studies were graded as high (4, 5), moderate (2, 3), or low quality (0-1) (see Tables 2 and 3 for details of all full-text manuscripts accessed and quality grading).
Data analysis
A random effects meta-analysis, using the DerSimonian and Laird Method,14 was employed on the individual study estimates to generate national and sub-national summary estimates of prevalence and risk of dementia in Nigeria. Standard errors were determined from the reported crude estimates and population denominators, assuming a binomial (or Poisson) distribution. Heterogeneity between studies was assessed using I-squared (I2) statistics, and subgroup analysis was conducted to detect causes of heterogeneity. A meta-regression epidemiologic model based on aggregated age from each study (as this was statistically significant) was applied to extracted prevalence rates. The model accounted for study sample size, study period, and estimated sex-based risk (for sex distribution). We employed the model to estimate the absolute number of cases of dementia at midpoints of the United Nation (UN) population 5-year age groups for Nigeria for the years 1995 and 2015.15 Our approach to data analysis has been described in detail in previous studies.16,17 All statistical analyses were conducted on STATA (Stata Corp V.14, Texas, USA). The study was conducted in strict compliance to the PRISMA guidelines.
RESULTS
Search results
Our searches returned 835 studies (MEDLINE 278, EMBASE 491, Global Health 58, and AJOL 8). Additional three studies were identified through Google Scholar, websites and reference lists of relevant studies. After duplicates have been removed, 440 titles were screened for relevance. On applying the selection criteria, 396 studies were excluded. Of the remaining 44 full-texts assessed, nine studies18–26 were finally selected for the review (Figure 1).

Study characteristics
Nine studies (7 population-based and 2 hospital-based) spread across the southern and northern parts of Nigeria were selected (Table 2). Specifically, six studies were retained from the South-west, two from the North-west and one from the North-central. Five studies were conducted in peri-urban settings, which we define as a mix of urban and rural dwellers. Four studies were rated as high quality, with the remaining five rated as moderate quality. Study period ranged from 1992 to 2017, with four studies (44.4%) conducted after 2010. The total population included in the review was 10,820, with a median age of 74.4 years (Table 3).
Estimated prevalence of dementia in Nigeria
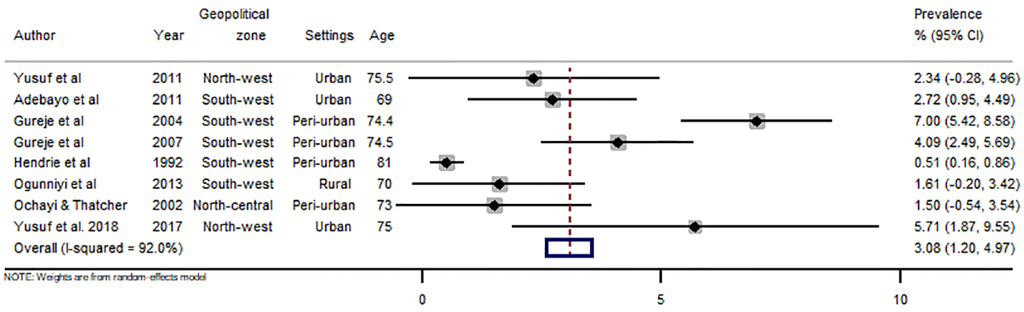
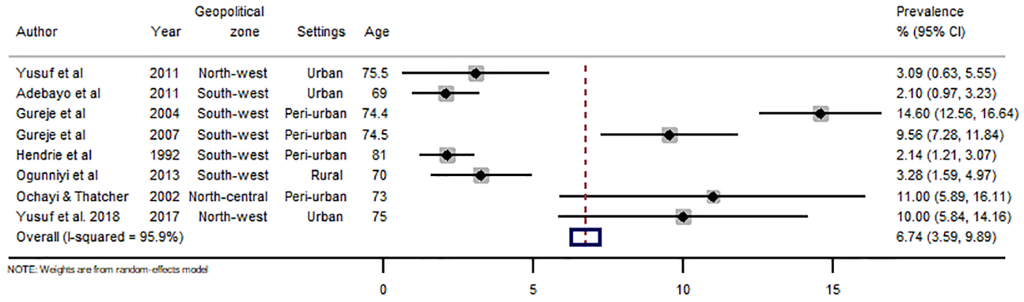
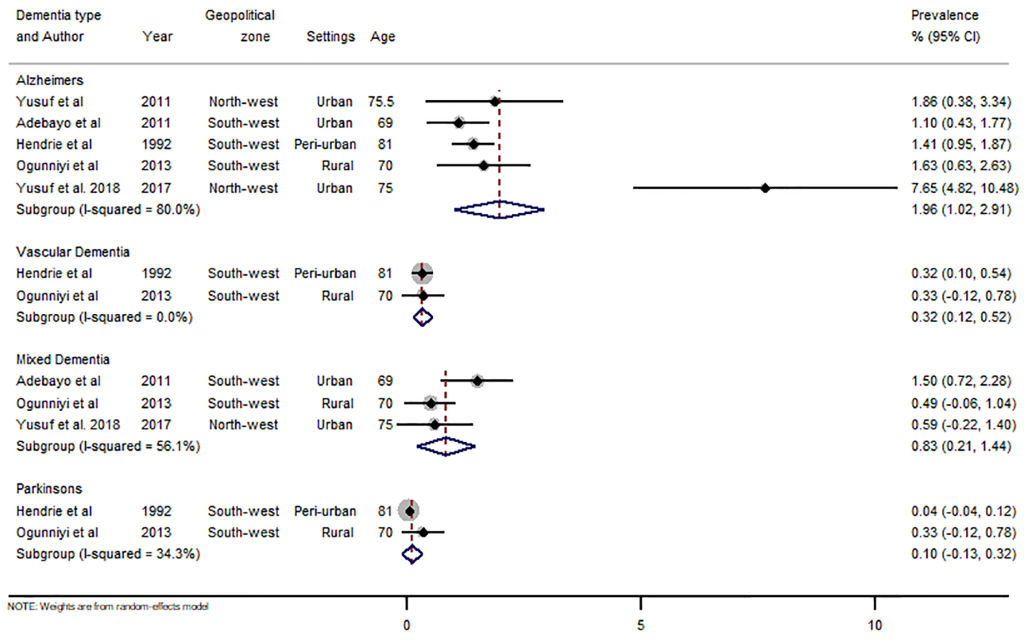
There were 43 data-points on the prevalence of dementia in Nigeria, 31 on dementia, five on Alzheimer’s disease, three on mixed dementia and two each on vascular dementia and Parkinson’s disease (see Online Supplementary Document(Online Supplementary Document) for all data points on prevalence). Heterogeneity was high across studies, with I-squared (I2) estimated at 98.8% (P<0.001). From all data points, the pooled crude prevalence of dementia in Nigeria was 4.9% (95% CI: 3.0-6.9) (Figure 2), with prevalence in women (6.7%, 3.6-9.9) significantly higher than in men (3.1%, 1.2-5.0), P<0.05 (Figures 3 and 4). The prevalence was highest in North-central (6.4%, 3.5-9.3), followed by North-west (5.4%, 0.1-10.7) and South-west (4.6%, 2.3-6.9). Prevalence was also higher in urban settings (4.9%, 2.5-7.4) compared to rural settings (2.8%, 1.5-4.1). As already reported as a disease associated with ageing, we observed an increasing prevalence with advancing age of the population, with prevalence consistently increasing from 3.9% (2.1-5.7) among persons aged 60-69 years to 11.0% (6.7-15.3) among persons aged 90 years or more (Table 4). Of the dementia subtypes, Alzheimer’s disease had the highest prevalence at 2.0% (1.0-2.9). Other dementia subtypes had prevalence rates less of than 1% (Figure 5, Table 4).




Estimated risk of dementia in Nigeria
We extracted data on 16 different risk factors yielding a total of 55 data points from all studies (see Online Supplementary Document(Online Supplementary Document) for all data points on risks). Of all extracted risk factors, age, female sex and BMI were significant determinants for dementia in Nigeria. At 80 years or more, the risk of dementia increased by almost 60% (odds ratio (OR) 1.58, 95% CI: 1.32-1.88). There was about 120% increased risk of dementia in the female sex (OR 2.18, 95% CI: 1.41-3.36), which is in keeping with our estimated prevalence rate distribution in the two sexes (male 3.1%, female 6.7%). Body mass index (BMI) 18.5 or less was also a leading risk of dementia observed in this study (OR 3.50, 95% CI: 1.22-10.05). Although, other contributing risks of dementia in a Nigerian population included being a widow (OR 1.47, 0.9-2.3), having no education (OR 2.36, 1.0-5.6), low socio-economic status (OR 1.52, 0.8-2.9), rural residence (OR 1.45, 0.8-2.9), history of alcohol (OR 1.51, 1.0-2.3), and history of stroke (OR 1.37, 0.7-2.5), they were however not statistically significant (Figure 6).

Estimated number of dementia cases in Nigeria
The meta-regression epidemiologic modelling, adjusted for study period (1992-2017) and sample size (total 10,820), was applied to mean ages and crude prevalence rates of dementia extracted from all studies. As noted in the prevalence estimates, the modelling revealed an increasing prevalence with age (P<0.05) (see Online Supplementary Document(Online Supplementary Document) for meta-regression model). Using the United Nations demographic projections for Nigeria and incorporating the significant female risk of dementia (to determine sex distribution), we estimated 63,527 dementia cases in 1995 among persons aged 60 years or more. Driven partly by the rapid demographic changes observed in Nigeria, this increased significantly to 318,011 dementia cases in 2015. This increase accounts for over 400% increase in the absolute number of dementia cases among persons aged 60 years or more over the 20-year period (Table 5).
DISCUSSION
Nigeria has one of the most rapid demographic transitions in Africa. A population health consequence of the associated population ageing is dementia. According to the UN estimates,15 the population of Nigerians aged ≥60 years nearly doubled from approximately 5 million in 1995 to 9.5 million in 2015. Thus, even if the existing age- and sex-specific prevalence of dementia remains stable, there will be an increase in the number of older individuals at risk of progressing into dementia.1,2
With dementia cases estimated at about 64,000 in Nigeria in 1995, it is compelling to suggest that the burden of dementia may have been previously low and gradually increasing in the country over the last two to three decades. In a 1992 study in Ibadan, South-west Nigeria, Ogunniyi et al.27 identified no cases of dementia in their study, reporting that the disease was relatively rare in Nigeria. Further studies in the same location21,22,28 gradually identified dementia cases, with the most surprising being a prevalence of 10.1% in 2006.19
We estimated an overall dementia prevalence of 5% (3.0-6.9) in Nigeria. To the best of our knowledge, this is the first national prevalence of dementia in the country based on a synthesis of diverse publicly available evidence. Our prevalence estimate is similar to that for Africa in the World Alzheimer Report for 2013 (4.6%) and 2015 (5.5%).1,29 However, Mavrodaris et al4 reported that prevalence rates of dementia in sSA ranged from 0% to 10.1%, and George-Carey et al5 estimated a dementia prevalence of 2.4% in sSA in 2012, which are both not in congruent with our current estimate. As these are aggregated estimates from different African countries where relatively little dementia research effort occurs, it is understandable that dementia prevalence may vary widely between, and even within, different countries.6
For example, genetic, cultural, and nutritional variation across the continent, and within African countries may have impacted the natural history of chronic disease prevalence, including dementia.6 This may be reflected in the different prevalence rates reported. Other factors that may have affected estimation include methodological issues, case definitions, validity and reliability of screening instruments, and under-reporting from routine medical records.5,8,13 In contrast, Prince and colleagues2 suggested that the actual prevalence of dementia only varies slightly between world regions, reporting a narrow range of 5-7% across countries, which appears to be in keeping with the World Alzheimer Report estimates for Africa and our current estimate for Nigeria.
We also estimated prevalence rates for dementia subtypes in Nigeria, with Alzheimer’s disease being the most prevalent at 2% (1.0-2.9). Alzheimer’s disease is the most common type of dementia globally and poses a substantial burden to patients, caregivers, and the health system.1 In sSA, George-carey et al5 estimated that Alzheimer’s disease accounted for almost 60% of dementia cases in the region in 2012. However, interpreting reported prevalence rates of dementia subtypes in Africa may need to be undertaken cautiously. First, due to apparent overlaps in the case definitions of dementia subtypes, particularly dementia, Alzheimer’s disease and vascular dementia, misclassification bias may have been a problem during case ascertainment.5 Second, dementia research is still evolving in Africa, with a relatively higher likelihood of errors from survey designs and use of screening instruments.4,8
Advancing age is the single most important risk of developing dementia, which was particularly significant for persons aged 80 years or more in this study. Although a decline in age-related incidence may be plausible with substantial reduction in exposures to other risks including environmental, lifestyle and cardiovascular risks.30,31 The increased risk of dementia in women observed in this study (from prevalence estimates and risk estimation) has also been reported previously.31 As women tend to live longer than men, they endure a survivor burden owing to higher prevalence of some diseases, such as dementia, especially when they have co-existing cardiovascular conditions.13 However, one important link is the presence of apolipoprotein E gene (APOE4 allele), a known risk of early-onset dementia, which creates proteins that transport fatty substances in the blood stream. Altman and colleagues32 found that women who carry a copy of APOE4 allele were twice as likely to develop Alzheimer’s disease, while men with the gene had only slightly increased risk, suggesting that APOE4 allele confers more risk of dementia in women compared to men. The link between dementia and BMI is controversial, hence our estimate of increased risk with BMI≤18.5 requires further research. Some studies have examined the association between weight and dementia, reporting that the risk of dementia increased among those overweight or obese.6,33 However, in a UK retrospective cohort study of about 2 million people over two decades, the authors reported that underweight people had a 34% increased risk of dementia compared to normal weight individuals and that the incidence of dementia consistently dropped with rise in BMI.34 While the contexts of these studies are obviously different from Nigeria, the contradicting reports further affirms a need for more research on BMI and dementia.
Although the Ibadan group have pioneered dementia research in Nigeria, it has been isolated mainly to South-west Nigeria. Further, few studies have addressed modifiable risks of dementia in the population, thus limiting population-wide guidance for the promotion of preventive measures.6 The lack of comprehensive care and support institutions for people living with dementia is another setback in Nigeria.35 Care for dementia is largely provided by family members and occasionally community care-givers. While better than no support, both groups suffer from a poor understanding of the disease and are burdened from the stress of providing care and the diverse behavioural disturbances of their loved ones. A bill to pass the Nigerian Mental Act, believed to potentially drive an improved response to dementia, was only re-introduced in 2013, having been withdrawn from the National Assembly for nearly five years due to unresolved political issues.7 The bill however broadly focused on protecting the rights of individuals with mental disorders and setting standards for mental health practice in the country. It is therefore important for policymakers to direct efforts at ensuring adequate infrastructure, personnel, training and research that focus on dementia, among other important mental health needs, in Nigeria.
This study has limitations. First, there were no studies specifically from the South-east, South-south and North-east of Nigeria that met our selection criteria. Second, study heterogeneity was high due to variation in study designs, case definitions, and individual population characteristics. The selection of two hospital-based studies could have also contributed to this heterogeneity; we however ensured these were properly screened and reference population clearly defined. Third, there were only four studies assessed as high quality, which obviously has implications on the interpretation of our results. Notwithstanding, the data and estimates provided in this study have been derived from the best available evidence on dementia in Nigeria and may contribute to better awareness and response to the disease in the country.
CONCLUSION
The prevalence and cases of dementia is increasing in Nigeria, driven mostly by rapid population ageing. There are still very few rigorous population-based studies on dementia prevalence and risk, and this apparently sustains a poor understanding of the diseases across many Nigerian settings. While there is need for the government and policy makers to address this issue more keenly, the country may also benefit from international collaborations towards advancing dementia research and overall mental health services in the country. It is hoped that the findings of this study may prompt a much-needed policy and public health response to dementia across Nigeria.
Acknowledgements
The authors acknowledge the support of the Nigeria Federal Ministry of Health and the WHO Nigeria Country Office in the conduct of this study.
Funding: None.
Conflict of interest: DA is a Co-Editor-in-Chief of the Journal of Global Health Reports. To ensure that any possible conflict of interest relevant to the journal has been addressed, this article was reviewed according to best practice guidelines of international editorial organizations. All authors have completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author). None of the participating authors has a conflicting financial or other interest related to the work detailed in this manuscript.
**Correspondence to:**
Dr. Davies Adeloye, MBBS, PhD
Centre for Global Health Research
Usher Institute of Population Health Sciences and Informatics
University of Edinburgh
MacKenzie House, 30 West Richmond Street
Edinburgh EH8 9DX, Scotland, UK.
[email protected]