In many regions around the world people are living longer and healthier lives. However, environmental pressures, climate change, population growth, and food security issues have created health problems that require a multidisciplinary One Health (OH) approach to finding solutions. One Health is the term that refers to the collaboration of multiple disciplines working locally, nationally, and globally to attain optimal health for people, animals, plants, and the environment.1 In this paper we outline one community-based approach to monitor and improve early detection of OH problems, to build human health capacity to solve those problems, address animal and plant health problems, and to harness the power of technology while also serving to identify emerging and re-emerging disease at an earlier period when early intervention will prove more effective.
We are constantly reminded of emerging and re-emerging zoonoses (Ebola virus disease, Middle East Respiratory Syndrome (MERS), Influenza A), and diseases in plant species (Taro leaf blight, wheat head blight, potato blight) that show how vulnerable plants and life sustaining agriculture are to disease.2–6 The majority (75%) of new and re-emerging human pathogens are zoonotic emerging from wild animal species.1,7 As the human population increases, people are forced to live in closer proximity to wild and domestic animals which forces the sharing of limited food and water supplies increasing exposure to new pathogens.8 To this, add the desire for generating new reveue by low-middle income countries through ecotourism which brings humans and animals into closer contact leading to the spead of illness, sometimes lethal, back and forth between humans and vulnerable wildlife. A recent example of this is the spread of human viral respiratory disease to vulnerable mountain gorillas (Gorilla beringei beringei).9
Infectious diseases are not the only OH concern affecting human, animal, and plant health.9 Waste and toxins dumped in, or near, water contaminate streams, rivers, and lakes affecting entire communities of crops, animals and people.10,11 Landscape alterations such as deforestation or algae blooms impact land quality, natural animal habitat, and erosion in areas. Beyond landscape changes, there are pressures to increase agricultural production, global warming with resultant changes in weather that decrease freshwater supplies, and changing microbial patterns that result in a deterioration of natural resources and the reduction in many of the protective ecological functions that maintain healthy ecosystems and benefit human, animal, and plant communities.12 Moving forward, a focus on promoting health depends on expanding from a uniquely human centric perspective to a broader OH perspective with attention on the interdependence between humans, animals, plants, and the environment.
There are key advantages of an integrated OH systems approach to reducing disease and managing ecosystems including:
-
engaging in the early and rapid detection of health threats;
-
collecting data to promote an integrated disease surveillance, prevention, and response system;
-
improving education and communication among professionals focused on human, animal, plant, and environmental issues to allow for earlier intervention;
-
exposing and integrating students engaged in professional education to concepts related to OH that facilitates inter-professional collaboration around discovery, innovation, and research;
-
developing policy focused on upstream drivers of disease emergence including land use and landscape alterations, water access and cleanliness, migration, and climatic shifts; and
-
strengthening the economy by improving long term impacts on food safety, security, and
- productivity.13–16
Community health workers
For decades, under various names (eg, Chinese barefoot doctors and Russian feldshers) and job descriptions, a group of minimally trained local workers have sought to function at the interface between community members and whatever health care system exists within a country.17,18 Today, around the world, in countries such as Rwanda, Ethiopia, Sri Lanka, and South Africa, community health workers (CHWs) have become the bedrock and frontline health care providers as they deliver or monitor treatments, engage in the detection of common illness such as malaria and HIV, or offer preventive care through immunization, and maternal and child health. CHWs could be the peripheral nervous system of a nation transmitting local information to a central processing center where executive decisions can be made, and early disease patterns and epidemics identified. At a central level the decisions made are carried back to the end organ – the community – in the form of treatments or early interventions. Today, these frontline CHWs function in their communities to provide limited primary preventive and curative services directed at humans but as a result of their job description little attention is given to the animal, plant, and environmental health interfaces.
CHWs have great potential to improve the health of a community but their job description needs to be broadened without significantly changing their mission. Despite decades of providing services at the frontlines, CHWs often still function in a grey area of health care delivery and are often under-trained with little support. This is where technology can be enabling. CHWs need additional training and supervision, access to high-quality health information, and technology such as mobile devices capable of providing just-in-time information and improved communication with higher level providers.19
Rural community’s limited access to veterinary health services has not only had a negative impact on livestock production with implications for food security, but has led to the inappropriate and indiscriminate use of antibiotics given to animals by lay people struggling to maintain their animals’ health 20 and increase productivity. Not long after the value of CHWs was realized by the human health community, non-governmental organizations (NGOs) began training teams of Community Veterinary Workers (CVWs) to deliver basic treatment to animals (eg, vaccinations, anthelminthics) in remote rural areas.21
In those same isolated rural areas, there have also been attempts to provide small commercial and family farmers with agricultural advice, often through agricultural extension programs aimed at increasing yield production and reducing the use of harmful pesticides.22 Poor field maintenance and failure to recognize common agricultural health problems results in the death or decreased crop production of important food sources.23 Inappropriate use of pesticides and other products that are toxic to animals and humans often enter the soil or water supply through misuse.24 This lack of health integration across human, animal, plant, and environmental health sectors in an ever-shrinking world with landscape degradation and decreased access to clean water begs for a shift in health services.
INNOVATIONS
A new paradigm for community health workers
Studies suggest enormous health benefits are derived from community workers.25,26 But, what if the CHWs job shifted from an entirely human focus to one with a one health focus to provide support across all four domains, human, animal, plant/crop, and the environment, to enhance health in the broadest sense 27? What if rather than being trained to deliver advice and treatment based on their own knowledge and memory recall, CHWs could rely on technology to provide evidence-based recommendations around human, animal and environmental/crop syndromes while also collecting and recording data that could be forwarded to referral centers, as well as to district or national disease monitoring centers for early outbreak detection and pathogen identification?
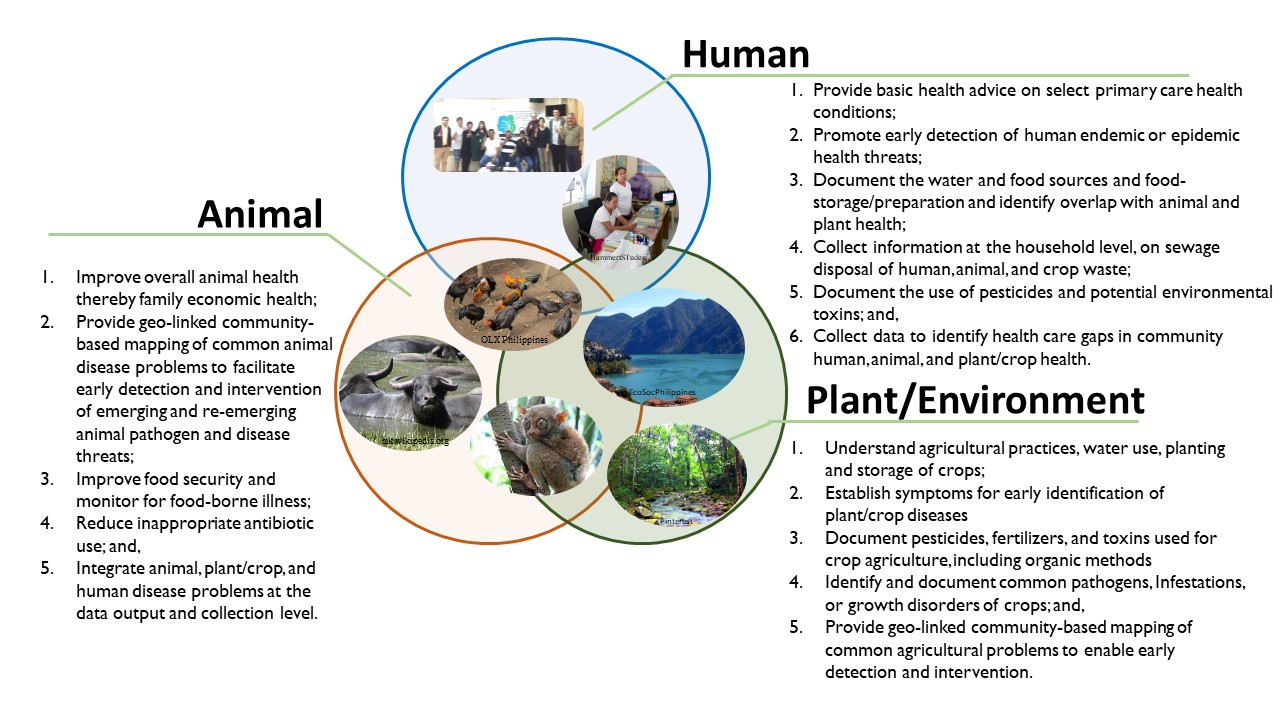
Globally, the World Health Organization (WHO) estimates that more than 400 million people lack access to health providers and basic healthcare services.28 This gap is far larger when considering access to veterinary health and agricultural services. To meet this challenge our international team has developed a human workforce innovation – a new model of CHWs termed a “One Health Worker” (OHW) with two objectives – 1) addressing basic human, animal, crop/plant, and environmental health issues at the community level, and 2) early identification of pandemic disease threats.29–31 The goals for carefully trained and supervised OHWs (Figure 1) are to 1) perform syndromic surveillance for human, animal, and plant diseases, 2) use technology assisted mobile devices to provide health advice and education at the household level, 3) use this same technology to collect and aggregate health data (animal, human, plant, environment) across regions to enable rapid detection of emerging diseases, and 4) facilitate the timely and appropriate referral to more advanced health professionals (human, animal, and plant) by providing an electronic record of all encounters.

Innovations in One Health
In most rural areas in low and middle-income countries the detection of, and response to, important diseases is slow and fraught with problems related to 1) collecting accurate data over wide geographic areas, 2) poor inter- and intra-professional communication, and 3) rapid aggregation of data into a useable format to show disease trends. The expanded use of mobile technology is a worldwide phenomenon both in and outside of healthcare. As availability of wireless access has improved mobile technology is being used to assist CHWs particularly related to delivering prenatal care and family planning services.32 Furthermore, mobile devices and a variety of software are accepted and valued by both CHWs and the public. Mobile health tools can provide rapid collection of data, collection of media rich data (videos, photos, audio, geo-positions), real time consultations, and professional supervision.
mHealth tools have been shown to guide health care workers through the collection of surveillance data and the dissemination of “just in time” prompts and recommendations, but this technology has not been utilized to provide data on diseases, or adverse health events, affecting human, animals, crops, and local environmental issues.33 Advantages of technology for providing “just-in-time” health guidance to OHWs include timelier care, a higher quality of evidence-based care, and more rapid resolution of problems including appropriate referrals. There are also enormous benefits in being able to geo-tag data through the global positioning system (GPS) to allow for the collection and surveillance and monitoring of incoming data related to humans, animals, and crops at the family and community level. We have developed a training course and an interactive mobile application (APP) with push and pull technology.
Our mHealth smart device APP is developed around a pictorially driven menu protocol with simple pattern recognition and does not depend on thousands of hours of experience or classroom teaching to build expertise that is needed for high level critical thinking. Rather, our APP distills expertise into manageable patterns such that relatively inexperienced workers with only a secondary education can use these tools to identify common and important syndromes, and notify trained professionals (eg, municipal level health, animal, and agriculture professionals) as needed. The APP menu is designed to be visually driven by photos, animations, and diagrams to aide in navigation. This tool can run either offline to circumvent problems with reliable internet access, or on a nation’s wireless telephone network to transfer data to a cloud server. The APP’s PULL technology collects geo-linked data from the OHWs input (via their APP) on OH problems.
Behind the scenes a web-based tool aggregates data input from all the OHWs and PUSHes that data out such that it can be combined with climate information (eg, temperature, rain fall) or other data, to create a geo-linked dashboard of syndromes that may indicate potential outbreaks. Each morning the dashboard displays problem areas for evaluation by municipal, regional, or national level agency experts, for possible early intervention and follow-up. For complex problems or serious outbreak concerns, messages, photos, and history of the problem can be sent by supervising nurses to the respective human, animal, or plant experts who can opt to advise the OHW via text message or pay a visit to the family in person. The advantage of our innovative system is that it can: 1) aid in providing surveillance coverage to a large area using existing human resources; 2) be easily scaled; and 3) includes numerous human, animal, and plant/crop diseases and management issues that impact the community and nation.
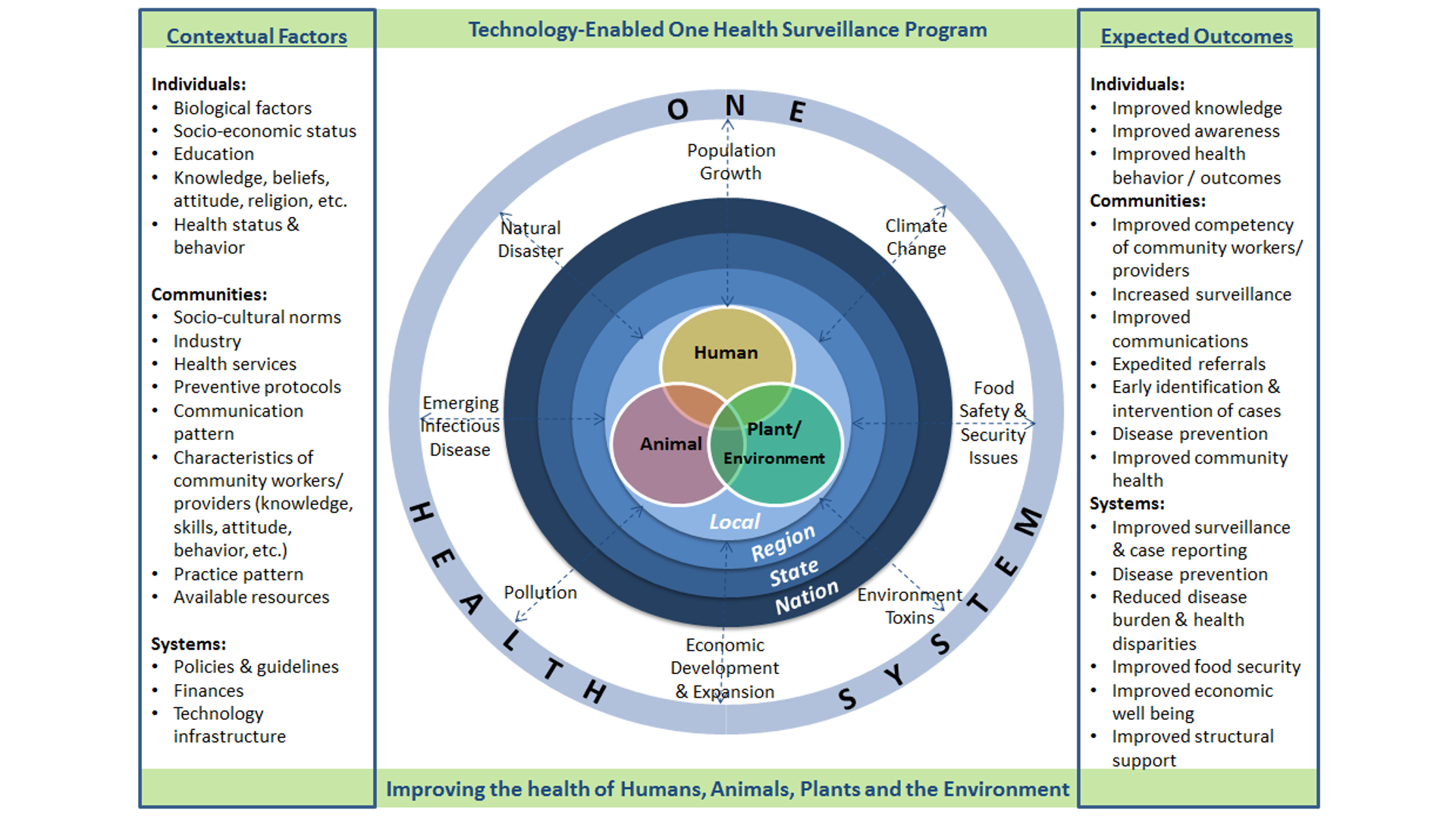
Conceptual model
The concept of holistically linking human, animal, environment, and plant/agricultural health issues is not new. As shown in Figure 2, there are multiple factors that impact one health at the animal/ecological/human level across the nation. Data is needed from a variety of sources to effectively and strategically determine interconnections across the domains, reduce disease burden and inform policy changes including early intervention of emerging disease threats. There is a vital role that can be played by OHWs as they engage in problem identification at the local level (Figure 2). Each community in which OHWs function has its own demographics and unique social and cultural norms that influence the acceptance of the OHW. Each community exists with its unique environmental issues including weather and water source concerns and may also include major employers/industries or recreational activities. It is this community that the OHW, assisted by technological tools, will be trained in communication skills, technology application, approaches to education and behavior change, and basic health knowledge so that they can provide grassroots linkages between the community and the formal human health care, animal, and agricultural management systems through collection and dissemination of health data. Each OHW will follow evidence-based protocols and report to advanced practitioners such as nurses, physicians, veterinarians, and agricultural officers. Easily interpreted data will then be aggregated and disseminated to regional and national experts who will engage in decision making to promote the health of the public and achieve a set of measurable outcomes.

TECHNOLOGY-ENABLED ONE HEALTH SURVEILLENCE IN THE PHILIPPINES
Philippines: Moving from CHW to OHW
The Philippine government, like many others, is faced with important health challenges including the shortage of well-trained, motivated, and equitably deployed health workers, particularly in geographically isolated rural regions where 56% of the population resides.34 Demands for living space, clean water, food security, animal health, crop productivity, and clean, inexpensive energy pose enormous social, political, and economic challenges that have significant impacts on human health and well-being.35 In this lower middle-income country with greater than 103 million people, 4% of the gross domestic product is allocated for health care, making equitable provision of health care a challenge.36 Large regions of the country have limited access to primary care and even fewer have access to expertise for animal or plant health. Further, rural populations often have no reliable form of transportation to access healthcare often located many kilometers away. There are other roadblocks, such as economic feasibility or infrastructure support (e.g. electricity, water systems), to building and staffing clinics or hospitals in rural areas. In terms of health indicators, the Philippines lags behind other Asian countries including India, Malaysia, Thailand, Vietnam, and Sri Lanka.37
In the Philippines the community clinic-based health worker is termed a “barangay (village) health worker” (BHWs). BHWs are local community members who take an 80-hour course focused on a small number of human health issues. They typically work within the community clinics except when they engage in specific community outreach programs such as village-wide immunization programs. Currently, BHWs are involved in promoting immunization, educating women about pre- and postnatal care, and in other programmatic efforts raising community awareness around child and maternal health. In the Philippines, BHWs have had mixed results, but overall, they show a moderate level of competence with a clear need and a strong desire for additional training and mentoring.38
Both in the Philippines, and globally, governments and NGOs have developed training programs that typically exclude concerns that are relevant to OH, including issues related to environmental pollution, toxins, zoonotic diseases, animal or plant health, water quality, and food safety and security. Lack of essential OH services in remote areas can lead to inadequate human and animal vaccination programs, decreased herd health and productivity, decreased crop production, and missed opportunities for the early intervention of disease outbreaks.
New methods of health improvement require a less reductionist and siloed approach and a more efficient and integrated approach that goes beyond focusing on one disease, one region, or even one species. The complexity of current health problems requires interdisciplinary expertise and a genuine cooperation of numerous governmental and nongovernmental agencies capable of understanding, monitoring, and engaging in collaboration to protect human, animal, and environmental health.39 No one scientific discipline, NGO, or governmental organization has the expertise or resources to address the emerging or reemerging threats to health. By breaking down barriers between disciplines and governmental agencies the Philippines government seeks to develop forward-looking solutions to meet its health challenges. Our strategy to address the health concerns of humans, animals, and plants/crops in rural areas is to develop a newly aligned community health workforce – a One Health Worker – who will work across the domains and provide these workers with technological resources.
Implementation of a One Health surveillance program
The Philippines government seeks to improve health through early detection, intervention, and monitoring of OH problems. One important step is the development of a OHW workforce guided by the training and technological resources based on internationally accepted evidence-based recommendations.
-
On the animal front, OHWs will use their mobile APP to collect data that will be useful to understand the community’s relationship with animals, approaches used in animal husbandry, management of animals used for food consumption, common animal illness and treatments including successes and failures, and methods of slaughter for food preparation and storage. The mHealth technology will provide algorithms for common animal problems, suggestions for interventions, and allow timely access to experts for concerns that are not routine or when suggested interventions have failed.
-
Many rural households have gardens or reside close to cultivated crops in the Philippines. In 2017, approximately 25% of the Filipinos were employed in plant agriculture that includes rice, coconuts, banana (abaca), corn, rubber, and many other fruits and vegetables.40 In the Philippines cultivation of these crops often demands fertilizer and pesticide use to manage pests and optimize crop yields. Even the use of organic fertilizers may contaminate food sources with zoonotic or environmental pathogens or contribute to leaching of pesticides and/or toxins into the environment.10 The OHW will identify patterns of specific pesticide or fertilizer use and help in the early detection of plant/crop diseases and/or crop failures. With the guidance of their mobile app, and access to agricultural expertise at the academic or district level, community-based OHWs will provide monitoring and advice for plants and crops.
-
On the human side of the OH triad, OHWs seek to narrow health care disparities as they engage in regular house to house surveillance for acute illness and provide health advice/education. OHWs will provide just-in-time health advice using the evidence-based mHealth device that guides them through algorithms, and ultimately to timely referrals to the appropriate provider (community clinic, district clinic, or hospital) with electronic data transmitted to the health care delivery facility.
CONCLUSION
To date, most attention around OH has focused on policy and academic problem-solving. Academic groups, government agencies, and NGOs can, and should, meet and engage in strategic planning around the resolution of complex global OH problems requiring inter-disciplinary expertise, cooperation, and creative problem-solving. However, practically, a OH approach needs to start at the community level where there is a strong need for OH data collection and health information dissemination. Our innovative OH approach has the potential to bring a new trained workforce equipped with mHealth technology to rural communities to improve the health of people, animals, plants, and the environment. Furthermore, the benefits of a OH workforce are vital for surveillance of emerging diseases and chronic health problems across all siloes. By the systematic collection of data, and the daily compilation of that data using geo-tagged mapping there is the potential to improve disease surveillance and detection, decrease lag time in response, and enhance monitoring of outcomes. Given the interconnectedness of our global community in which humans, animals, plants, and the environment impact each other and do not respect geopolitical boundaries, we believe it is time for countries to consider training a community-based OH workforce.
Acknowledgements
None.
Funding
Philippine Government (PCARI) IIHTM 16.
Competing interests
The authors have completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author), and declare no conflicts of interest.
Correspondence to:
Michael Wilkes, MD, PhD
School of Medicine, University of California, Davis
1 Shield Ave, Davis, CA 95616
USA
[email protected]